Vaccine Hesitancy on the Rise
/Further evidence of the current attack on science is the opposition to vaccination against infectious diseases such as measles, hepatitis and polio. More and more parents are ignoring science by choosing not to vaccinate their children, even with vaccines that have a long history of extensive testing for adverse health effects. The WHO (World Health Organization), for the first time, listed so-called vaccine hesitancy as one of the top 10 global threats in 2019.
According to a new poll from health policy information nonprofit KFF, 16% of U.S. parents have skipped or delayed vaccinating their children against diseases other than COVID-19 or the flu during the 2024-25 school year. The same poll reveals that white parents, Republicans, the religious and those who homeschool their kids are more likely to avoid the shots.
Data for the MMR (measles-mumps-rubella) vaccine exemplifies vaccine hesitancy. The KFF poll found that only 92.5% of U.S. kindergarteners received the MMR vaccine in 2024-25, a significant drop from 2019-20 when the percentage was 95%.
The reason this drop is significant involves herd immunity. Herd immunity is the mass protection from an infectious disease that results when enough members of the community become immune to the disease through vaccination, just as sheer numbers protect a herd of animals from predators. Once a sufficiently large number of people have been vaccinated, viruses and bacteria can no longer spread in that community.
The threshold for herd immunity, which is the minimum percentage of the population that needs to be vaccinated for the herd effect to take hold, depends on the contagiousness of the disease, the effectiveness of the vaccine and other factors. For highly contagious measles, herd immunity requires up to 95% of the populace to be immunized, while for polio the percentage ranges up to a slightly lower 86%.
KFF reports that 39 U.S. states had MMR vaccination rates for kindergarteners below the target rate of 95% for the 2024-25 school year, an increase from just 28 states during the 2019-20 (pre-pandemic) school year. And of the 39 states, 16 reported even lower rates of below 90% for 2024-25, compared to only 3 states in 2019-20; the particular states are shown in the figure below. (Montana and West Virginia didn’t report data for the 2024-25 school year).
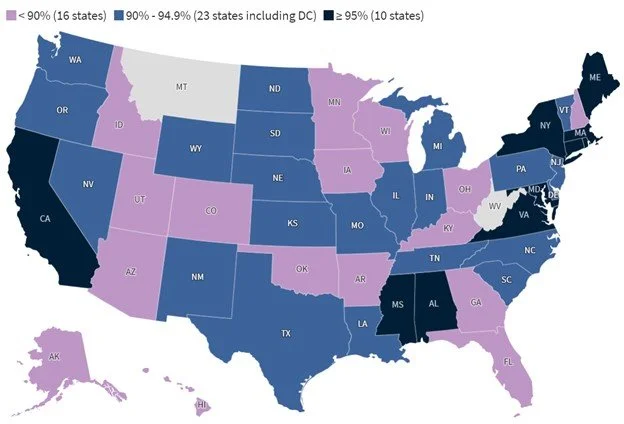
MMR coverage rates among kindergarteners for the latest school year varied widely from state to state: from a low of 78.5% in Idaho to a high of 98.2% in Connecticut. In 2024-25 alone, over half the states experienced declines in vaccination rates for all state-required vaccines, including MMR, DTP (diphtheria-tetanus-pertussis), polio, and chicken pox.
One of the factors contributing to this decline in vaccination rates is exemptions from mandatory vaccination, both religious and philosophical, the latter exemption being based on strongly held personal, moral or other nonreligious beliefs. Although fewer U.S. states allow philosophical exemptions than grant religious exemptions, all 50 states provide exemptions on medical grounds.
The share of U.S. children claiming an exemption from one or more vaccinations rose from 2.5% in the 2019-20 school year to 3.6% in 2024-25. However, the increase comes from an increase in nonmedical exemptions; medical exemptions actually decreased slightly over this interval.
The uptick in exemptions is clearly visible in the next figure, which displays the number of states with exemption rates in select percentage groups by school year, for one or more vaccines. While fewer and fewer states are reporting exemption rates below 3%, the number with exemption rates above 5% is on the rise; this means that those states cannot reach the target vaccination rate of 95% for the MMR vaccine, even if all nonexempt children receive their vaccinations.

But religious and genuine philosophical exemptions constitute only a small fraction of overall objections to vaccination. By far the greatest number of objections come from those who are fearful of side effects or do not trust vaccine safety. Vaccine hesistancy is also fueled by widespread misinformation, including misunderstandings about herd immunity.
It’s true that serious adverse reactions to a vaccine shot do occur occasionally – typically about once in every million vaccinations. But this is a minuscule risk compared with the risk of contracting the disease itself in an unvaccinated community during an epidemic.
Unvaccinated children exposed to someone infected with measles, for instance, have a 90% chance of contracting the disease, and one of 1,000 children who get the measles will develop encephalitis, an often debilitating aftereffect that can lead to seizures and mental retardation. That’s a risk of about one in 1,100 of experiencing a serious aftereffect for a child who comes down with measles, compared with the much lower risk of one in one million following vaccination. Some children still die from measles, often after getting pneumonia.
Science tells us that it’s much more risky for a child to forgo vaccination and suffer the consequences of catching a potentially deadly disease, than to be vaccinated against it.
Next: Past Global Warming Was More Rapid than Today’s: The Younger Dryas